|
|
Achondroplasia
General Considerations
- Autosomal dominant or sporadic mutation disorder of abnormal enchondral bone ossification
- Most common form of short-limbed dwarfism (less than 3rd percentile in standing height)
- In achondroplasia, the extremity involvement is rhizomelic (i.e. proximal) so that the humerus and femur are more involved than the radius and tibia.
Clinical Findings
- Delayed motor development
- Recurrent otitis media
- Normal intelligence
- Short stature
- Lower extremity radiculopathy
Imaging Findings
- Can be detected before birth by the use of prenatal ultrasound
- After birth, conventional radiography is the study of first choice
- Skull
- Frontal bossing
- Enlarged calvarium and mandible
- Hypoplasia of the midface
- Hands and feet
- Short phalanges
- Fingers of equal length (trident hand)
- Spine
- Narrowing of the interpediculate distance
- Thickening and shortening of the pedicles
- Decreased height of vertebral bodies
- Anterior wedging may produce a “bullet” shape
- Pelvis
- Squared iliac wings
- Narrow sacroiliac notches (Champagne glass appearance)
- Reduced acetabular angle
- Long bones
- Bones are short (rhizomelic) and wide
- Genu varum
- Widening of the metaphyses
- Posterior bowing of the distal humerus
Differential Diagnosis
- Diastrophic Dysplasia
- Spondyloepiphyseal Dysplasia
Treatment
- Somatotropin (recombinant human growth hormone), especially during years 1-6 of life, may be helpful
Complications
Prognosis
- Life span is usually normal
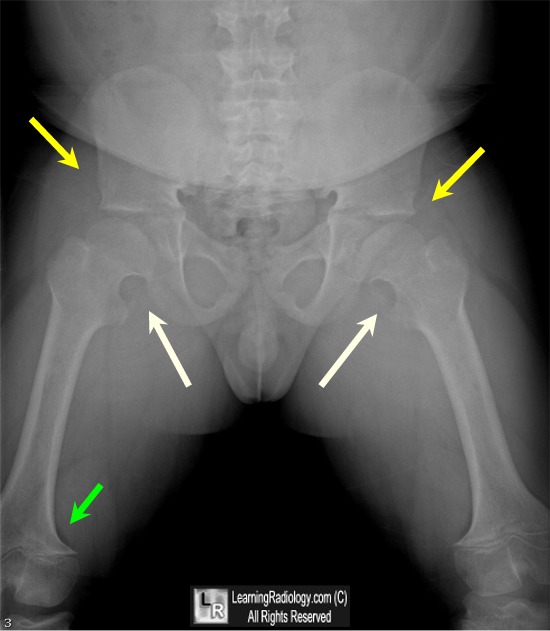
Achondroplasia. Note squaring of the iliac wings (tombstone pelvis), flattening of the acetabular angles (yellow arrows), genu varum deformities (white arrows) with widened but shorter femurs and flaring of the metaphyses (green arrow). Inner pelvis is shaped like a champagne glass.
For more information, click on the link if you see this icon 
Achondroplasia. Shital Parikh. eMedicine
|
|
|
